The Impact of Traumatic Life Events: Reactions and Resilience – Part I Abstract
Featured Article

The purpose of this article was to review the impact of traumatic life events on individuals in today’s world. The Bible has indicated that such events were the result of Adams’ sin. The article explored the scope of traumatic life events and the psychological impact they can have on persons exposed to them. Individuals vary in their response to experiencing trauma incidents which ranges from common to chronic posttraumatic reactions, such as Posttraumatic Stress Disorder. Resilience was also defined in relation to traumatic life events. Finally, several positive resilience behaviors were identified that can help individuals prevent and reduce the impact of encountering a traumatic life event.
The Impact of Traumatic Life Events: Reactions and Resilience
Traumatizing life events have been occurring ever since Adam’s choice to disobey God (see Genesis 3). In fact, the Spirit of Prophecy penned, “Adam was tested in a very simple manner, but his failure to endure the test opened the flood-gates of woe upon our world” (White, 1888, par. 5). Hence, from the world-wide catastrophic flood found in Genesis 7; to the volcanic destruction of Pompeii and Herculaneum in 79 AD; to the terrorist attacks of September 11, 2001; to the devastation caused by Hurricane Katrina in 2005; to the destructive earthquakes that struck Haiti in 2010 and more recently in Rio, Italy in 2016; to the 2004 Indian Ocean and 2011 Japan tsunamis – not to mention the countless number of wars and skirmishes that have occurred – provide a snapshot of evidence that testifies to the “woe” that humankind has experienced since the Fall. Unfortunately, the price that these disastrous events bring also include the potential development of psychological after-effects among those who experience them (Norris, Friedman, Watson, Byrne, Diaz, & Kaniasty, 2006; Neria, Nandi, & Galea, 2008). Therefore, the purpose of this article is to: (1) briefly describe the scope of traumatizing events; (2) define the common reactions that are associated with experiencing a traumatic life event; (3) describe resilience and its importance in the context of trauma; and (4) conclude with several suggestions that one can implement to help mitigate the negative impact of a traumatic life event.
The Scope of Traumatizing Life Events
In order to understand the impact of a traumatizing life event one must first define what it is. In a nutshell, traumatic life events or “critical incidents” (as often referred to in the crisis intervention literature) are specific, unexpected, time-limited, events that involve loss or a threat to one’s physical and psychological well-being (Everly, Flannery, & Mitchell, 2000). Table 1 provide examples of traumatizing life events.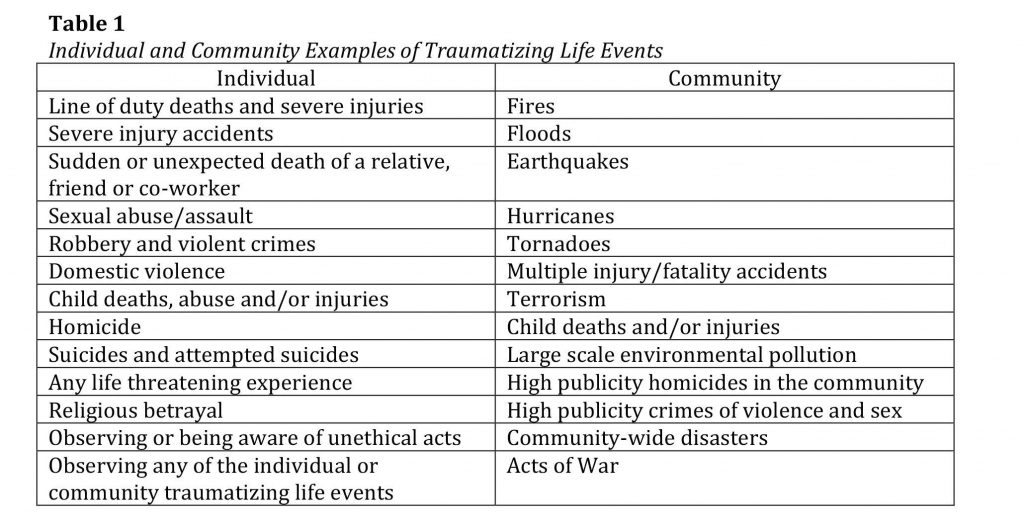
The reality of such traumatizing life events can be observed in the statistical data collected to report the extent of their impact. For instance, in 2014 Guha-Saphir, Hoyois and Below (2015) reported that worldwide naturals disasters killed 7,823 people, with an economic cost of $99.2 billion and contributed to over 140 million people becoming victims. Furthermore, 2014 recorded 13,370 terrorist incidents in 93 countries, resulting in 32,685 deaths (Global Terrorism Index, 2015). In the United States, it has been estimated that 50% to 60 % of its citizens have been exposed to traumatic stressors (Ozer, Best, Lipsey, & Weiss, 2003), with about one fifth of individuals possibly experiencing such an event within any given year (Nandi & Vlahov, 2005). Raphael (1986) has suggested that at least 25% of the population may be affected, which in turn, may contribute to a 15-25% surge in demand for mental health services (Everly, 2015).
The Impact – From Common to Chronic Reactions to Traumatizing Life Events
As previously illustrated, experiencing traumatic life events is not surprising or uncommon. Although a large number of people may be exposed to traumatic life events individual reactions will vary, are common and often transient, with the majority of people being able to resolve the trauma with limited or no disruption in their ability to function on a day-to-day basis (Bonanno, 2004; Shalev, 2002). As a matter of fact, Myers and Wee (2005) cited several research studies that posit full recovery from moderate stress reactions within 6 to 16 months for the majority of individuals who experience a traumatic life event. The commonality of such posttraumatic symptoms has led many disaster behavioral health responders to use the phrase, “you are experiencing normal reactions to an abnormal event” to help reassure trauma survivors that their reactions to the event are universal. Table 2 provides several categories that have been used to describe a subset of commonplace stress reactions after experiencing a traumatic situation.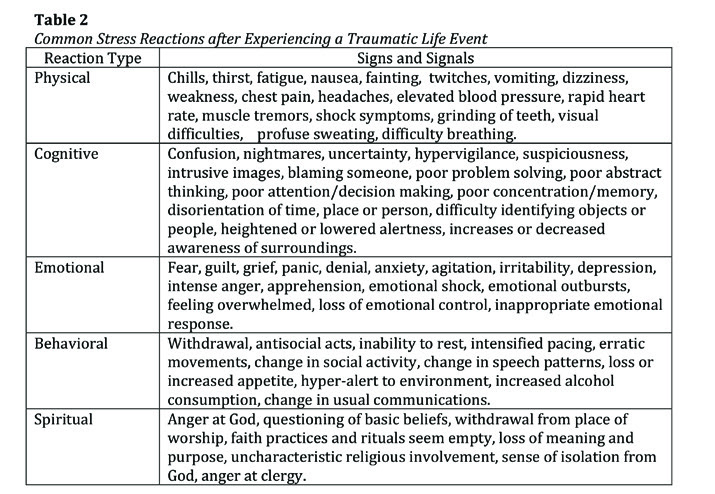
Unfortunately for some people, undergoing a traumatic event, whether directly as a victim or vicariously as a witness, may place such individuals in a state of psychological crisis that impairs coping behaviors that can lead to increases in alcohol consumption, depression and/or the development of more debilitating mental health problems (Everly, Flannery, & Mitchell, 2000; Flannery, 1994; Keyes, Hatzenbuehler, & Hasin, 2011). Moreover, studies have consistently shown that the proximity of exposure to a traumatic event is linked to the development of a more chronic mental health problem known as Posttraumatic Stress Disorder (PTSD) (Galea et al., 2005; Norris et al., 2002).
PTSD has been classified in mental health circles as an anxiety disorder that can develop among children and adults after exposure to a traumatic life event, and is followed by characteristic symptoms of intrusive recurrent distressing memories or dreams of the event, avoidance behaviors, negative changes in thinking and mood, and hyperarousal/hypervigilance. Symptoms must occur for more than one month and need to be of sufficient severity to interfere in important areas of functioning in a person’s life (i.e., chronic absenteeism from work or increased risk taking behaviors). PTSD has been associated with several predictors which include having a history of prior trauma, prior psychological adjustment problems, a family history of psychopathology, perceived life threat during the trauma, posttrauma social support, peritraumatic emotional responses, and peritraumatic dissociative experiences (Ozer, Best, Lipsey, & Weiss, 2003).
In regards to the prevalence rates of PTSD, meta-analysis research has estimated lifetime prevalence at around 7% (Ozer et al., 2003), with a 12-month prevalence among adults in the U.S. at roughly 3.5% (American Psychiatric Association, 2013). Ozer and her colleagues have also indicated that since 50% or more of the U.S. population is exposed to traumatic life events, only 5% to 10% will develop PTSD. Higher rates of PTSD are often common among professions with increased risk of exposure to traumatic events (e.g., veterans, police, firefighters, and emergency medical personnel), with the highest rates among survivors of interpersonal violence, such as rape, military combat and captivity, politically motivated confinement, and genocide (APA, 2013; Skogstad, Skorstad, Lie, Conradi, Heir, & Weisaeth, 2013).
Harvey J. Burnett, Jr, PhD is the Chair of Behavioral Sciences Department,
Andrews University, Berrien Springs, Michigan
[Editor’s note: This is the first part of Dr. Burnett’s article. The conclusion will appear in the November-December issue of the Journey to Life]